
{kind=link}
Those who follow me on X, the hellsite formerly known as Twitter, know that I just spent the last few days in Orlando (unfortunately) to attend the annual meeting of the American Society of Breast Surgeons. You might also know that I stirred the pot a bit on social media by posting my objection to the keynote speaker citing what I like to call a zombie statistic, namely that long-debunked claim that medical errors are the third leading cause of death in the US, accounting for over 250,000 deaths annually. Unfortunately, the stirring didn’t take, but if you want to know why this zombie statistic is bogus but nonetheless won’t die and, worse, seemingly has become part of accepted wisdom, a statistic thrown out at the beginning of so many medical talks as though it were accurate, read this. Moreover, the real number is likely 5- to 20-fold lower. I even thought about writing an update looking at the latest evidence regarding the death toll from medical errors, but decided that that was a project that would require more time than I had last weekend, between travel, meetings, and the like. File it away for later, in favor of something that I can handle fairly quickly but still caught my interest.
I’ve now written more times than I can remember why the antivax claim that COVID-19 vaccines are causing a wave of “turbo cancers” is utter nonsense. Briefly, the idea is that somehow the evil humors in the vaccine are more powerful than the most powerful known carcinogen (ionizing radiation) and have caused a wave of highly aggressive cancers in only three years since the vaccines were even widely administered. Never mind that most cancers take more like 10 years to show up after exposure to a carcinogen and that the ones being reported (mostly solid tumors like breast, colon, etc.) do not match the few cancers types that can appear less than three years after exposure to a carcinogen, like leukemias. I thought I had seen every twist on the “turbo cancer” myth; that is, until this weekend.
You see, another meeting was going on last week, overlapping the breast surgery meeting. It’s a meeting that I used to go to every year but, since the pandemic, have not attended. I’m referring to the American Association for Cancer Research (AACR). This year, I had to choose, and unfortunately it made more sense to choose a clinical meeting. In any event, there was a talk presented at the meeting that found that the incidence of “accelerated aging”—I’ll explain how that was defined in a moment, when I get into the weeds of the study that I could find, even though it hasn’t been published in a peer-reviewed journal yet—has increased in younger cohorts of adults. If confirmed, it would be a very interesting finding, something worthy or further research to determine why this might be happening. It might also potentially be an explanation for why the incidence of cancer has been increasing in younger people over the last 25 years.
Quote antivaxxers: It’s got to be the vaccines that done it!
Of course, that’s not how antivaxxers saw it, and the news reports in even conventional media didn’t help. Before I get to the abstract itself, let’s look at the AACR press release, entitled, blandly enough, Accelerated Aging May Increase the Risk of Early-onset Cancers in Younger Generations. Basically, the finding was that accelerated aging was more common in recent birth cohorts and was associated with increased incidence of early-onset solid tumors. SciTech Daily’s headline tacked onto the press release was a little more provocative but not particularly alarming, Unraveling the Rapid Aging Mystery Behind Early-Onset Cancers. ASCO Post reported, Accelerated Aging May Be a Risk Factor for Early-Onset Cancers in Younger Generations, while CNN added, Accelerated aging linked to cancer risk in younger adults, research shows. You can probably see where I’m going with this and how antivaxxers decided to spin the study, which, again, hasn’t even been formally published yet.
First, there was the NY Post headline, Cancer rates rising in young people due to ‘accelerated aging,’ according to ‘highly troubling’ new study. Note the “highly troubling” part added. Also note that this article was actually by Melissa Rudy of Fox News. It also, for no apparent reason other than to fear monger, quotes Dr. Brett Osborn, portrayed as an “expert in longevity.” Never having heard of Dr. Osborn before, naturally I just had to Google him. Unsurprisingly, this is what I found near the top of the search results:


And:
To Brett Osborn, DO, FAANS, CSCS, most ailments of modern-day society can be prevented. The West Palm Beach neurosurgeon, author, and founder of Senolytix views good health as a privilege to be earned.
“Patients should not expect their doctors to keep them in good health,” he says. “Most patients could solve their problems by taking simple steps, like losing weight, exercising more, and eating better.”
Dr. Osborn founded Senolytix to help put patients on a path to extend the number of years of optimal body and mental health. From comprehensive assessments of a patient’s condition, he develops a plan built around better nutrition, proper exercise, and medications that may include hormone replacement therapy, supplements, and improved sleep.
On his website, he makes it even more explicit:
The following are the most important:- Health is a privilege, NOT a right.- There are no “diets,” or secret exercise regimens which will grant one health or a particular body type. Proper manipulation of one’s biochemistry through the above modalities (i.e., turning on the right genes through strength training) will grant one health and longevity.- Health is a lifelong endeavor. There are no races. It is a lifestyle. We must constantly strive to better ourselves (through daily physical and mental challenges) in order to delay the aging process.- Keep bodily inflammation at a minimum (through strength training, nutrition and supplementation, proper sleep and stress reduction techniques). This maintains nearly all disease processes in check.
Good health is a “privilege to be earned”? Seriously? This is the sort of attitude that is everything that is wrong with “alternative health.” What about people who are not sufficiently privileged to be able to adhere to a program like the ones that Dr. Osborn promotes? What about people with genetic predisposition to disease that they inherited through no fault of their own? No one is saying that lifestyle changes, such as a healthier diet and getting more exercise and better sleep, can’t be very beneficial to health, but these people seem to engage in a combination of magical thinking that people have complete control over their health and whether they get sick or not. (“This maintains nearly all disease processes in check”? At least he said “almost.”) Unsurprisingly, like most medical “entrepreneurs,” Dr. Osborn has a YouTube channel, a Twitter feed, and other social media where he hawks his company Senolytix, which offers all sorts of tests and “longevity” medicine interventions. Oh, and his father, whom he cites as an inspiration, was a chiropractor.
My point is simply that he is clearly not a real expert on the science that was reported at AACR. Being boarded by the American Academy of Anti-Aging Medicine is not a qualification of which I’d be proud. If you don’t believe me, just search for this organization on this blog.
I don’t want to dwell too much on Dr. Osborn’s take, though. Rather, I mention it mainly to show how a mainstream news organization quoting an anti-aging entrepreneurial neurosurgeon with an agenda, someone who dogmatically states:
NO ONE is too old for strength training. NO ONE is exempt from exercise. Numerous studies have demonstrated that one’s ability to combat disease is resident within our muscles. Muscles are the protein depots from which our immune system indirectly generates antibodies. Stronger individuals live longer, period. This HAS been proven.
Actually, there is indeed such research, but that same research shows that there are other factors associated with longevity. As we say, it’s complicated.
In any case, it’s a spin on the findings like that of Dr. Osborn that really is just a short hop, skip, and a jump to someone like Mike Adams in a story like Government comes up with another new excuse for the genocide they’ve unleashed upon the planet: ‘accelerated aging’ among the young is causing all of these ‘turbo cancers’, complete with an image like:

Let’s see how he spins these findings. After that, I’ll go through the study to tell you what the investigators really found, so that you can see how quacks cherry pick unpublished studies from meeting proceedings and spin them into, well, something like this.
Hilariously, this isn’t even original Mike Adams. He’s republishing an article by someone named Stefan Stanford republished at AllNewsPipeline.com, with an added tagline, “Eugenicists Covering Up Genocide To Avoid Being Executed For Crimes Upon Humanity.” Nice.
Behold:
The latest mind-boggling story over at the NY Post on Tuesday proving just how full of ‘s’ our ‘globalist overlords’ and the mainstream media are in 2024 is titled “Cancer rates rising in young people due to ‘accelerated aging,’ according to ‘highly troubling’ new study.”
Reporting that new research presented this week at the American Association for Cancer Research (AACR) Annual Meeting in San Diego, California has found that ‘the young’ are now aging much more rapidly than they have in the past and thus, they are being struck much more frequently with problems that had normally been mainly associated with ‘the elderly,’ take note that once again, these globalist scum are trying to come up with an excuse for the genocide they’re carrying out that should, in any kind of ‘just’ society, leave them all executed and buried 6′ under for their crimes upon humanity.
Reporting that ‘accelerated aging,’ when someone’s biological age is greater than their chronological age, is increasing the risk of deadly cancer tumors in ‘the young,’ we warned just days ago in this story on ANP that so-called ‘turbo cancers’ were exploding among younger generations, with Dr. William Makis MD warning us he had never seen anything like this before.
And while the globalists continue to come up with one excuse after another for this ‘explosion‘, such as ‘global warming‘ or ‘bacteria in the gut linked to processed foods,’ Dr. Makis ties the huge spike in these cases of rapidly spreading cancers in the young directly to the ‘COVID vax.‘
One more time, Dr. Makis is an antivax quack, and “turbo cancer” is not a thing. Moreover, let’s just say that the above take is a…highly exaggerated…version of what the study found, as you will see. Elsewhere, there are articles on quack antivax websites with headlines like, WEF-Linked Study Blames ‘Accelerated Aging’ for Spike in Turbo Cancers Among Young People. I note that the study said nothing about “turbo cancers.”
Meanwhile, on social media:
In fairness, there is another contingent blaming the “accelerated aging” on COVID-19, which is more plausible, but still overblown, given that such trends do not happen over a time period as short as the four years since COVID-19 hit.
But what did the study actually show?
“Accelerated aging”?
I almost hesitated to write this post because (1) I didn’t attend AACR and therefore didn’t attend the talk. Thus, all I have are the abstract, press releases, and news reports of interviews with the first author, Ruiyi Tian, MPH, a graduate student at Washington University in St. Louis, and her PhD thesis advisor in whose lab she did the work, Dr. Yin Cao, an associate professor of surgery and senior author of the new research; and (2) I don’t have the figures or detailed methods. I thought about it, though, and then figured that I do have enough to discuss that it should quickly become obvious that antivaxxers are just making stuff up about this research. Also, I’m sure it’s likely disconcerting to Ms. Tian and Dr. Cao; so if either of you see this post and want to chime in or ask for advice on what to do with antivaxxers swarming, let’s just say my email is [email protected].
So here’s the abstract:
The first thing to note is that this study took advantage of the UK Biobank. As I was unfamiliar with this particular database, I took a look at the UK Biobank website, to see that it is an impressive piece of work:
UK Biobank participants have generously provided a very wide range of information about their health and well-being since recruitment began in 2006. This has been added to in the following ways:
- Imaging: Brain, heart and full body MR imaging, plus full body DEXA scan of the bones and joints and an ultrasound of the carotid arteries. The goal is to image 100,000 participants, and to invite participants back for a repeat scan some years later.
- Genetics: Whole genome sequencing for all 500,000 participants, whole exome sequencing for 470,000 participants, genotyping (800,000 genome-wide variants and imputation to 90 million variants).
- Health linkages: Linkage to a wide range of electronic health-related records, including death, cancer, hospital admissions and primary care records.
- Biomarkers: Data on more than 30 key biochemistry markers from all participants, taken from samples collected at recruitment and the first repeat assessment.
- Activity monitor: Physical activity data over a 7-day period collected via a wrist-worn activity monitor for 100,000 participants plus a seasonal follow-up on a subset.
- Online questionnaires: Data on a range of exposures and health outcomes that are difficult to assess via routine health records, including diet, food preferences, work history, pain, cognitive function, digestive health and mental health.
- Repeat baseline assessments: A full baseline assessment is undertaken during the imaging assessment of 100,000 participants.
- Samples: Blood & urine was collected from all participants, and saliva for 100,000.
That’s a heck of a lot of data to mine. I can see why this database was attractive to Tian and Cao. One shortcoming of the study, though, is immediately apparent (and mentioned in a number of places). This is a UK-only study. Whether its results are generalizable to other populations is an open question. I also did some searches and found that there was a study by a different group using the UK Biobank published a year ago that showed correlation between a different set of biomarkers related to aging and the risk of developing cancer. What this study does that’s different is to try to quantify the risk of early onset cancers in people with elevated biological age as assessed by the nine biomarkers included in the PhenoAge calculator.
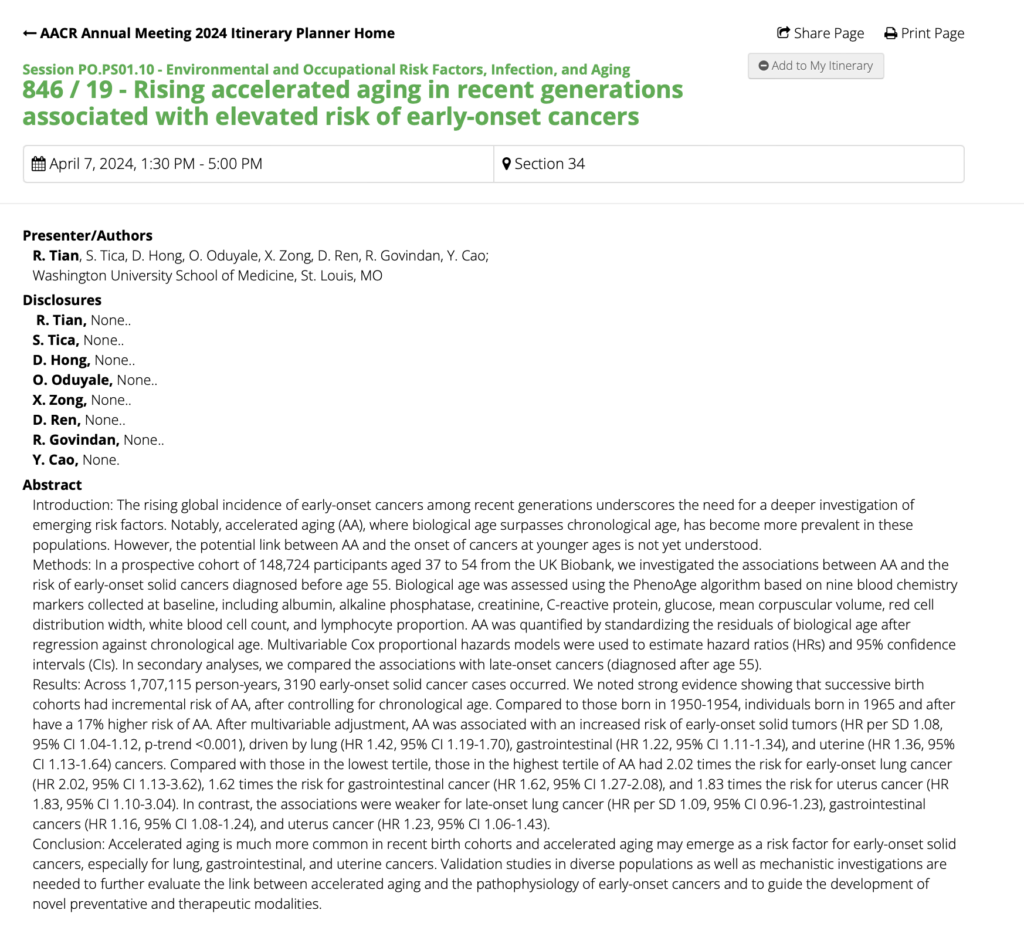
Next up, how was “accelerated aging” defined? Here’s how:
Biological age was assessed using the PhenoAge algorithm based on nine blood chemistry markers collected at baseline, including albumin, alkaline phosphatase, creatinine, C-reactive protein, glucose, mean corpuscular volume, red cell distribution width, white blood cell count, and lymphocyte proportion. AA was quantified by standardizing the residuals of biological age after regression against chronological age. Multivariable Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs). In secondary analyses, we compared the associations with late-onset cancers (diagnosed after age 55).
To put it more simply, nine biomarkers were examined, and an algorithm used to calculate each person’s “biological age” as indicated by these markers and compare it with their chronological age. CNN Health actually gives a good explanation of the relevance of each of these markers:
They homed in on nine blood-based markers that have been shown to correlate with biological age:
- albumin: a protein made by the liver that declines with age
- creatinine: a waste product in blood produced by protein digestion and the breakdown of muscle tissue; a measure of kidney function. Lower levels correlate with better longevity.
- glucose: With age, blood sugar stays higher for longer after meals.
- c-reactive protein: made by the liver in response to inflammation; relatively higher levels correspond to faster aging
- lymphocyte percent: The concentration of these white blood cells related to immune function tends to decrease with age.
- mean cell volume: a measure of the average size of red blood cells, which increases with age
- red cell distribution width: the difference between the size of a person’s smallest and largest red blood cells, which tends to increase with age
- alkaline phosphatase: an enzyme produced mainly by the liver and bones that tends to increase with age
- white blood cell counts: Numbers of white cells in the high end of the normal range in the blood may correspond with greater aging.
I do, however, feel obligated to point out one thing. PhenoAge is just one algorithm. It purports to measure “biologic age,” but does it? Does it really? That, too, is a weakness of the study. There is, of course, evidence that PhenoAge is better predictive of age-related health outcomes, such as all-cause mortality, cancers, healthspan, physical functioning, and Alzheimer’s disease, than other measures. It would have been nice to look at other potential measures of biologic age besides a single algorithm. One also can’t help but note that it would be a lot less sexy to say that a panel of biomarkers predicts your risk of early onset cancer than it was to say that “accelerated aging” does.
Moving on, CNN actually summarized the findings of the study pretty well:
They then checked cancer registries to see how many in the group had been diagnosed with early cancers, which the researchers defined as cancers appearing before age 55. There were nearly such 3,200 cancers diagnosed.
The researchers found that people born in 1965 or later were 17% more likely to show accelerated aging than those born from 1950 through 1954.
Basically, people who are currently younger than 59 have a 17% higher chance of showing signs in this panel of accelerated aging than those aged 70-74. This has consequences. Overall, for all cancers, people with accelerated aging have an of developing cancer with a hazard ratio (HR) of 1.08, but this was driven primarily by a few cancers, such as lung cancer (HR 1.42), gastrointestinal (HR 1.22), and uterine cancer (HR 1.36). Moreover, those with the highest degree of accelerated aging had the highest risk of early onset cancer, as high as two-fold (lung cancer).
So what does this all mean? One thing that it doesn’t mean is that COVID-19 vaccines are causing an epidemic of “accelerated aging” that is in turn causing an epidemic of early onset “turbo cancers.” These sorts of changes in biomarkers don’t happen overnight in a population, and a little over three years since the start of the mass vaccination campaign against COVID-19 is basically overnight. Also, again, it must be emphasized that cancers in response to carcinogens don’t pop up overnight, as the whole “turbo cancer” narrative claims. They take several years, usually a decade or more. Only some of the hematological malignancies take a timeframe under three years, and even then, even if COVID-19 vaccines were as cancer-causing as someone like Dr. Makis claims, we would only just now be starting to see an uptick in a small number of specific hematologic malignancies.
What is interesting about this study, if its results are replicated and bear out, is that they suggest a potential set of blood tests that could identify people at a higher risk for lung, GI, and uterine cancers, as well as a less dramatically elevated risk of other cancers. In other words, testing for accelerated aging could be a way of identifying people who are at higher risk, so that targeted interventions can be developed and implemented to decrease their risk.
What might explain these results and why these specific cancers seemed to be the most influenced by accelerated aging? One possible explanation:
The study wasn’t designed to answer questions about why these cancer types seemed to have the strongest ties to accelerated aging, but Ruiyi Tian, the graduate student who led the research, has some theories.
Tian said it’s possible that lungs are more vulnerable to aging than other types of tissues because the lung has a limited ability to regenerate. Stomach and intestinal cancers, she says, have been linked to inflammation, which increases with aging.
Not vaccines.
As an oncologist says:
Dr. Anne Blaes, who studies the impact of biological aging in cancer survivors at the University of Minnesota, said the study results are exciting because they could point to a better way to find people who are at higher risk of getting cancer when they’re young. Right now, young adults who don’t have a family history or other risk factor aren’t regularly screened for most kind of cancer.
“We’re seeing more and more cancers, especially GI cancers and breast cancers, in younger individuals. And if we had a way of identifying who’s at higher risk for those, then really, you can imagine we’d be recommending screening at a different time,” said Blaes, a professor and director of the Division of Hematology and Oncology at UM medical school. She was not involved in the new research.
Blaes said that if you can find people who are at higher risk because their cells are aging faster, you can target lifestyle interventions too: things like nutrition, exercise and sleep.
“There are medications that also look like they can slow down accelerated aging,” said Blaes, who is testing two of them in cancer survivors. Cancer survivors often show greater biological aging, perhaps because of the after effects of therapies like chemotherapy and radiation.
The medications belong to a class called senolytics, drugs thought to target and get rid of damaged and aging cells.
Of course, this reminds me of Dr. Osborn, whose company is called Senolytix, but let’s just say that, just perusing his website, I am less impressed with his dedication to rigorous science, although his website is quite slick and he does conveniently have three different levels of patient access, Express (meet the nurse practitioner, not Dr. Osborn), Essential, and Elite VIP (“our most extensive, full-service, VIP Concierge membership,” complete with full access to Dr. Osborn, “dependent on Dr. Osborn’s capacity & Neurosurgery call schedule,” of course). I note that the Elite VIP membership offers what many dubious anti-aging clinics that I’ve seen over the years have offered
That and his fear mongering in the NYP article didn’t impress me with his dedication to science:
“Our nation’s health – let alone Britain’s – is imperiled, and unless radical measures are taken, this trend will likely worsen before it gets better,” he warned.
“The younger population will be stricken with lethal diseases at an earlier age.”
Maybe, but what does he mean by “radical measures”? Never mind. I don’t care, for purposes of this discussion. He fits in mainly because of how Fox News used him as a dubious “expert” who promotes infrared saunas as longevity tools in order put an alarming spin on the story. From there, disinformation merchants picked up on it. Of course, antivaxxers and others promoting quackery have long been skilled at distorting and misappropriating legitimate research in order to promote a narrative supporting antivaccine views and quackery. This was just a particularly egregious one. It doesn’t matter that there’s zero evidence, either in this study or anywhere else, to support the false claim that COVID-19 vaccines are responsible for the phenomenon observed in the study so badly distorted by Mike Adams and his ilk.